
- Suite 1335, 13/F.,
Central Building,
1-3 Pedder Street,
Central, Hong Kong MTR
Central Station (Exit G) - 3104 0802


- |


- |

-
Suite 1335, 13/F.,
Central Building,
1-3 Pedder Street,
Central, Hong Kong MTR
Central Station (Exit G) - 3104 0802
- Home
- Central Line

Central Line
化療導管
Central Line
What is central venous access ?
Central veins are large veins inside the chest directly connected to the heart. Compare with the peripheral veins of the arms, they are much larger in diameter and has a much higher rate of blood flow. Medicine that is too concentrated or irritating to the peripheral veins may be administered directly into a central vein and become diluted very quickly. Central venous access provides for frequent intravenous infusion without the repeated painful needle sticks and surrounding inflammation. It makes the months of chemotherapy much less painful and less traumatic.
Use of central venous access
- Deliver chemotherapy in cancer patients
- Deliver coagulation factors in patients with haemophilia
- Deliver antibiotics to patients requiring them for a long time
- Deliver intravenous nutrition at high concentration
- Withdraw blood sample for test
Approach for the central vein catheterization
There are three common approaches for central vein catheterization:
- Subclavian vein (SV) lies just below the clavicle at the top of chest. It is the traditional approach
- Internal Jugular Vein (IJV) lies just above the clavicle at the base of the neck. It is the newer and the preferred approach
- Common femoral vein (FV) lies in the groin. Feasible but in an inconvenient position. It is the last approach
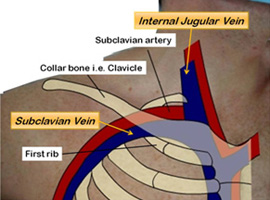

Catheter through the internal Jugular vein is the preferred approach
- IJV runs a straight course towards the right atrium. Mal-position is significantly less common with the jugular approach
- IJV vein is superficial, easily visualized with ultrasound. With the use of ultrasound to guide the needle puncture. Jugular approach has a much less risk of pneumothorax
- SV approach has a higher risk of puncture of an incompressible artery and bleeding is far more difficult to control
- SV is situated in between two bone (clavicle and rib), Long-term scissoring of the catheter inside the SV by the bones can damage the catheter (pinch off syndrome)
Type of long-term central venous access
- Partially implanted catheter
- Hickman line
- Boviac line
- Totally implanted injection port

What is an injection port?
The major users of implanted port are oncology patients. Most ports are placed below the collarbone on the chest wall by a vascular surgeon. The port provides a point of entrance into the central vein for infusion of medicine or withdrawal of blood. It is a self-sealing silicone bubble for repeat needle insertion. As silicon is a very inert material, rejection and allergy are not an issue.


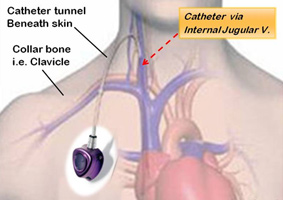
Implantation of injection port
A portacath is a type of central venous catheter, or central line. This is a long hollow tube, usually made of silicon rubber. It is placed into one of the large veins in the body. One end of the catheter is inserted inside a large vein, usually near to the heart. The other end of the catheter is attached to the port which is positioned just beneath the skin on the front of the chest, below the clavicle (collar bone). The port is felt as a lump under the skin and injections can be given via the port.
- The operation is carried out under full sterile conditions
- Skin of the operation site is cleaned with anti-septic solution
- Local anaesthetic is injected to numb the area
- Using the ultrasound the internal jugular veins is located
- Guided by ultrasound image, a needle is inserted into a central vein
- A small incision the "insertion site" is made around the puncture
- A fine metal wire is then threaded through the needle into the vein
- Position of the wire is checked with an X-ray
- A 'pocket' is created under the skin in the chest
- A port of the size of a 5 dollar coin is inserted
- A tunnel is prepared under the skin from the "insertion" site to the pocket "the exit site"
- A long silicon tube "a catheter" is pulled from the exit site through the tunnel to the insertion site
- The catheter is then passed over the wire and is guided into the central vein
- The port in the pocket is then connected to the catheter and buried beneath the skin
- The port appears as a bump under the skin
- The two sites are covered with water-proof dressing
- Patients hardly have any discomfort and can resume normal activity right after the implant



How to use the port?
Feel for the bump and locate the portal, then apply anaesthetic cream to numb the skin. Straight aseptic technique is used. A non-coring needle (Huber Needle) is inserted through the skin, then the septum of the port and into the port reservoir. The injection fluid flows from the reservoir through the catheter and into the patient's vascular system. The tip of the catheter is placed to a large central vein for maximum dilution of the infusate.

Advantage of injection port over indwelling line such as Hickman® line
- Do not affect daily activities
- It is completely internal so swimming and bathing are not a problem.
- Accepatable in appearance
- Totally implanted underneath the skin and require no special maintenance
Complications of central line insertion such as Hickman® line
- Pneumothorax - Attempts to gain access to the central vein can injure the lung, leading to air being trapped between the lung and the thoracic cage (pneumothorax). If it is large, chest tube need to be placed to remove the trapped air. In experienced hands and under guidance of ultrasound view, this complication is rare.
- Arterial injury - Artery and vein are close together and the artery can be inadvertently punctured. This usually leads to a subcutaneous hematoma. Higher risk of puncture of an incompressible artery during subclavian approach and bleeding is more difficult to control
- Infection - infrequently severe infection require the catheter to be removed
- Thrombosis - blood clot in the catheter may block the device. To prevent clotting the device is flushed with saline and heparin
- Mechanical failure –though extremely rare, it is possible that part of the system (in particular the subclavian catheter) could break and become lodged in the circulatory system.
- If the catheter stay in the vein for a long period of time there is a risk that the vein becomes narrowed